The service of General Surgery at the National Center for Minimally Invasive Surgery has had the greatest experience in laparoscopic procedures nationwide for 15 years, having performed over 13 000 surgical interventions. During this period, the faculty of teachers, certified and recognized to perform basic and advanced laparoscopic procedures, has introduced a great amount of new surgical techniques in Cuba, given the solid training and education received at the Cuban School of Surgery and laparoscopy. This education has grown due to training and courses at high level Centers from all over the world such as: the section of Minimally Invasive Surgery, School of Medicine , Eberhard Karls University, Tübingen, Germany; Telesurgery European Institute in Strasbourg and Clermont Ferrand International Center for Endoscopic Surgery in France; Hospital Clínico de Barcelona, Spain; Saint Pierre Hospital in Brussels, Belgium, among others.
Bariatric Surgery | Heller cardiotomy | Cholecystectomy | Colectoly | Splenectomy | Fundoplications | Inguinal Hernioplasty | Parietal Pleurectomy | Lung or Mediastinum, Pleural Mass Resection | Transthoracic sympathectomy | Adrenalectomy
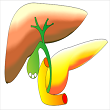
Comprises the following diseases that could be concomitant::
Gall bladder lithiasis
Common bile duct lithiasis
Intrahepatic lithiasis
The standard surgical procedure for biliary lithiasis is Laparoscopic Cholecystectomy, while the
common bile duct can be treated with Endoscopic Sphyncterotomy or by laparoscopic approach. Other
diagnostic procedures are required such as ERCP (Endoscopic Retrograde Cholangiopancreatography) and
LIOC (Laparoscopic Intraoperative Cholangiography).
Physician Team:
Rafael Torres Peña, MD. PhD.
Miguel Angel Martínez Alfonso, MD. PhD.
Javier E. Barreras González, MD. PhD.
Rosalba Roque González, MD. PhD.
Jorge Pereira Fraga, MD.
Hiran de Zacarias Rodriguez Blanco, MD.
Sigifredo de la Caridad Montero Ferrer, MD. PhD.
Raul Jimenez Ramos, MD. Ms. C.
Contact: tursalud@cce.sld.cu

Esophageal achalasia is the most frequent motor disorder; it is considered a disease of unknown etiology. It is characterized by the absence of peristalsis in the body of the esophagus and the incapacity of the lower esophageal sphincter to relax in response to swallowing. This gives rise to dysphagia (this word comes from Greek, literally meaning difficulty to eat) both solids and fluids; regurgitations; loss of weight are the most frequent symptoms with a marked deterioration of the quality of life of those who suffer from it. The procedure of choice at our center to treat the symptoms of patients diagnosed with Esophageal Achalasia is by laparoscopic surgical procedure, i.e. modified Heller´s esophago-cardiomyotomy, usually in addition with an ant reflux procedure, either Dor or Toupet.
Physician Team:
Miguel Angel Martínez Alfonso, MD. PhD.
Rafael Torres Peña, MD. PhD.
Rosalba Roque González, MD. PhD.
Jorge Pereira Fraga, MD.
Raul Jimenez Ramos, MD.
Contact: tursalud@cce.sld.cu

The disease due to gastroesophageal reflux (GERD) is a morbid condition that develops when the reflux
of gastric content causes annoying symptoms, complications or both. GERD is an important public health
issue. GERD management first requires medical treatment. The universally accepted surgical technique
is funduplication, with its different variants (total or partial). Laparoscopic surgery has the
unquestionable advantages of minimally invasiveness, such as: short hospital stay, less postoperative
pain, less morbidity and a fast comeback to daily life, among other advantages.
Laparoscopic funduplications have been performed in Cuba at the Center for Endoscopic Surgery,
currently, the National Center for Minimally Invasive Surgery, since 1994.
Physician Team:
Dr.C. Miguel Angel Martínez Alfonso
Rafael Torres Peña, MD. PhD.
Rosalba Roque González, MD. PhD
Jorge Pereira Fraga, MD.
Raul Jimenez Ramos, MD.
Contact: tursalud@cce.sld.cu

Inguinal hernia has an incidence in Cuba of 10 patients per medical office (i.e. out of every 400 to 500 patients). The prevalence is 15 out of the same number of patients; the occurrence worldwide is similar.
We are experienced in performing a laparoscopic approach for hernias at our Center.
EPhysician Team:
Jorge Pereira Fraga, MD.
Ana Bertha López Milhet, MD.
Hiran de Zacarias Rodriguez Blanco, MD.
Raul Jimenez Ramos, MD.
Contact: tursalud@cce.sld.cu

There have been three limiting factors for the development of colorectal laparoscopic surgery: its technical complexity, the increasing costs and the doubts regarding the oncological criteria respectability in the case of colorectal cancer.
Video laparoscopic management of patients who have: Video laparoscopic management of patients who
have:
Physician Team:
Rafael Torres Peña, MD. PhD.
Miguel Angel Martínez Alfonso, MD. PhD.
Jorge Pereira Fraga, MD.
Ana Bertha López Milhet, MD.
Raul Jimenez Ramos, MD.
Contact: tursalud@cce.sld.cu
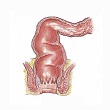
Colorectal cancer has become a health problem in the western world. It is the third most common cancer in the United States and represents 10% of cancer deaths in the United Kingdom (1). Meanwhile, the mortality rate associated with colorectal resections can be between 0% and 20% (2).
At our institution, benign and malignant rectal lesions are approached by Transanal Endoscopic Microsurgery (TEM).
Physician Team:
Rafael Torres Peña, MD. PhD.
Miguel Angel Martínez Alfonso, MD. PhD.
Javier E. Barreras González, MD. PhD.
Jorge Pereira Fraga, MD.
Contactar a: tursalud@cce.sld.cu
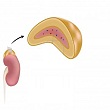
Adrenal glands can be ideally approached by laparoscopy. The reported advantages in this procedure
are less postsurgical ileus, fewer analgesics, shorter hospital stay, earlier postsurgical recovery
and better cosmetic advantages.
The first laparoscopic adrenalectomy was performed in our country at Hermanos Ameijeiras Hospital, in
1997. This procedure was later introduced at the National Center for Minimally Invasive Surgery,
improved and standardized after a collaboration agreement was signed with the Institute de Recherche
contre les Cancers de l’Appareil Digestive (IRCAD-EITS).
In 2001, the National Institute of Endocrinology and the National Center for Minimally Invasive
Surgery begin to work together in the management of these conditions.
Physician Team:
Rafael Torres Peña, MD. PhD.
Tania González León, MD. PhD.
Contact: tursalud@cce.sld.cu
Bariatric surgery is a treatment for the management of obesity that basically consists in reducing
the capacity of the stomach and altering the intestinal route by means of different techniques
(gastroplasty, gastric bypass, gastric band, etc.) in order to avoid fat absorption during the
digestive process.
Until recently, this surgery was performed by means of large incisions (laparotomy) and with high
mortality and subsequent disease rates.
At present, the patient is operated on by laparoscopic surgery through small incisions where all the
instruments, such as the camera and lights, are inserted. They will allow the surgeon to operate
inside the abdominal cavity with great precision, thus achieving a faster recovery of the patient,
minimal post-surgical pain, short inability period and minimal damage to the abdominal wall.

Sleeve Gastrectomy
It is a surgical procedure that consists of extracting approximately 80% of the stomach volume. A pipe-shaped stomach is left with a capacity of about 150-200cc. Weight loss is achieved by such an important reduction of the stomach volume, so it is a restrictive surgery.

Gastric Bypass
Gastric bypass is a surgical procedure which achieves weight loss by two mechanisms. On one hand, a stomach is made with a much reduced capacity (20-50cc), and on the other hand, a crossing (bypass) is made in the small intestine which causes that only 60% is used for digestion and absorption of food. This procedure has both a restrictive and a malabsorptive component, so it is considered a mixed gastric bypass technique.

Laparoscopic Gastric Plication
This surgery consists in the reduction of stomach volume by means of an inward fold (invagination) of the stomach wall. The original volume is occupied by the invaginated stomach walls so less food is allowed into the stomach. It is a restrictive surgery.
Physician Team:
Miguel Angel Martínez Alfonso, MD. PhD
Rosalba Roque González, MD. PhD.
Jorge Pereira Fraga, MD.
Raul Jimenez Ramos, MD.
Contact: tursalud@cce.sld.cu